 企業(yè)郵箱
企業(yè)郵箱






Pathomorphological Changes of Deep Burns Wounds Treated with
作者:Rong Xiang Xu 出版社:KARGER 發(fā)行日期:In 2004INTRODUCTION
BRT with MEBT/MEBO has been in wide use for many years domestically and internationally [1, 2]. Although many clinical practices have confirmed its advanced and scientific results in burns management, the mechanism involved in the healing of deep burns wounds without hypertrophic scar is not yet clear. From March to November 1994, the authors treated 12 patients sustaining deep burns with MEBO and performed light- and electron-microscopic observations on wounds before and after MEBO treatment. The aim was to explore the therapeutic effectiveness of MEBO on the healing of deep burns wounds.
MATERIALS AND METHODS
Twelve patients sustained 2-98% total body surface areas (TBSA), including 2-82 % third-degree burns. Most patients had burns mainly on the face and extremities and one patient was complicated with inhalation injury. Some patients suffered extremely severe burns covering the whole body skin. Areas which received MEBO treatment included chest, back, upper arm, thigh, leg, and instep. MEBO was applied on burns wounds in accordance with the standardized MEBO protocol.
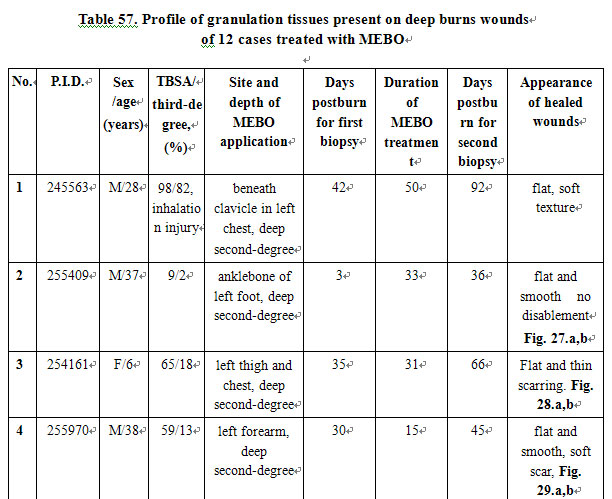
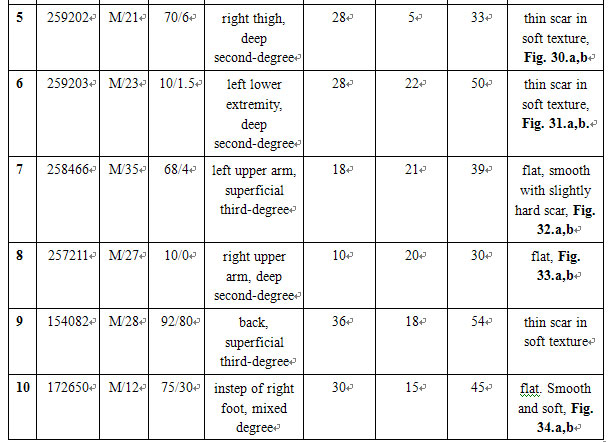
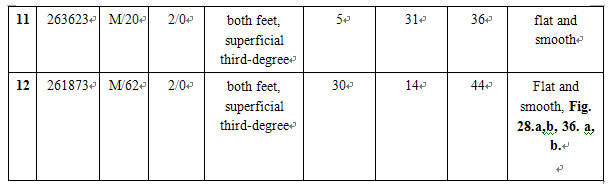
All of these patients were initially treated by conventional surgical therapy in other hospitals. Therefore, this study focused on deep second-degree and superficial third-degree burns wounds with intermediate and late granulation tissue on days 3-42 postburn that were treated with MEBO. The ointment application lasted as long as 5-50 days and the wound healed on days 30-92 postburn. Macroscopic observation of healed wounds showed the coverage of soft, flat and smooth epithelium or soft and flat scars, without the appearance of hypertrophic or contractive scars.
Consent to receive MEBO treatment was obtained from patients or their guardians. Two wound tissue samples 1 -2 mm3in size were taken from each patient before and after treatment. One of the samples was fixed with 75 % alcohol before being transferred to the pathological department for hematoxylin and eosin staining and light microscope examination (Olympus). The other was fixed with 2.5 % glutaraldehyde and 1 % osmic acid, stained with uranium acetate and lead citrate, and gradient dehydrated with ethanol and acetone. The ultrathin sections were examined under a transmission electron microscope (CM 10, Philips).
RESULTS
Light Microscope: The third-degree burns wounds penetrated to beneath the dermis and subcutaneous tissue that appeared as uniform pink necrosis. Some of the muscular tissue was also involved, where cross-striation of striated muscle disappeared and had the appearance of the pink color of coagulated necrosis. Infiltration of inflammatory cells presented around the sweat glands and hair follicles. During the course of treatment, collagenous fibers were found to proliferate severely, showing thick and disordered arrangement at the beginning. These progressed to moderate proliferation with thin fasciculi, and finally had the appearance of being delicate and orderly. After healing, the epidermis recovered to normal, and neoregenerated blood capillaries and fibrocytes appeared in the dermis (Table 57).
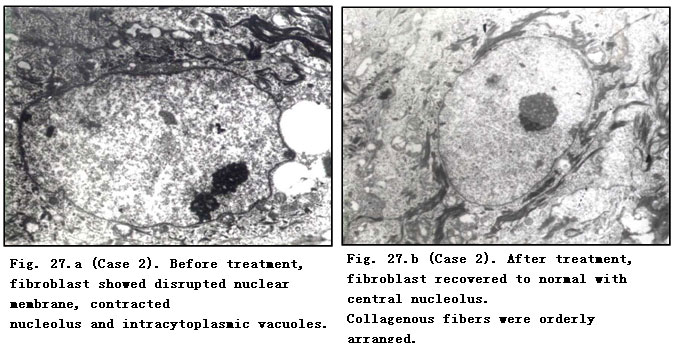
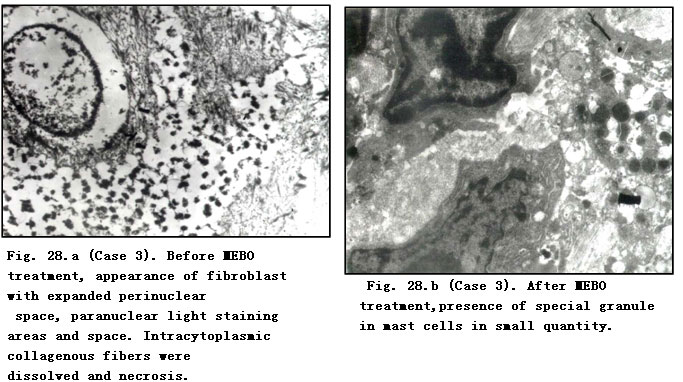
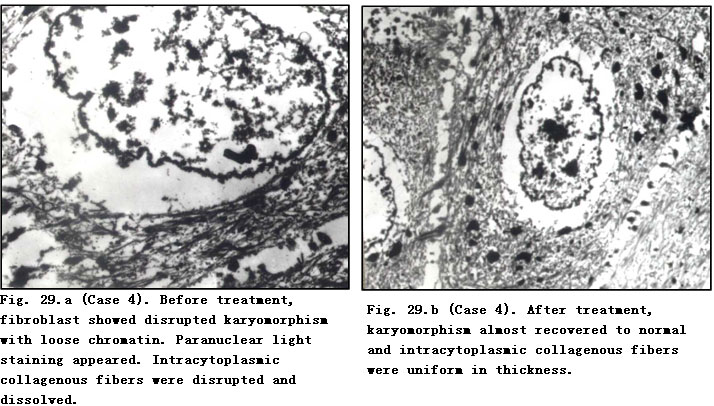
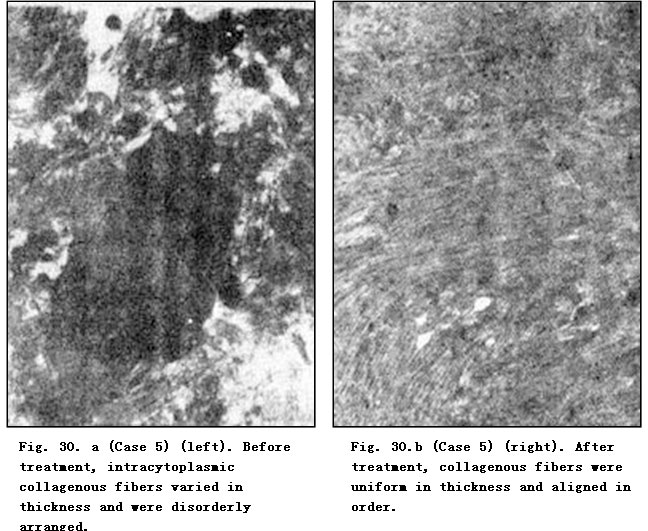
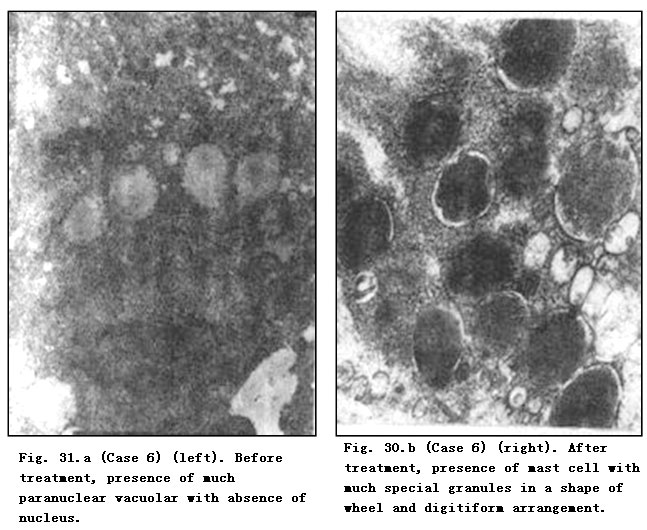
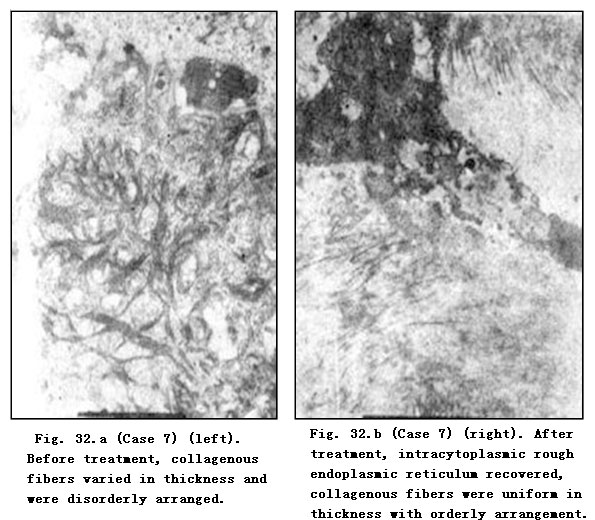
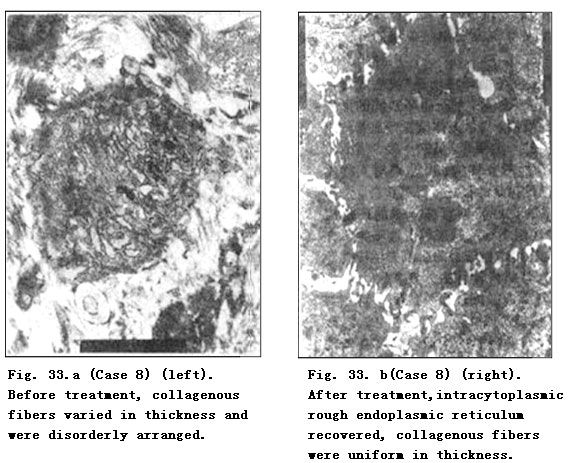
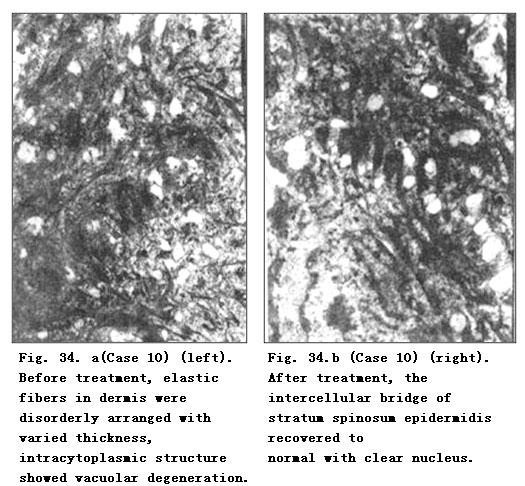
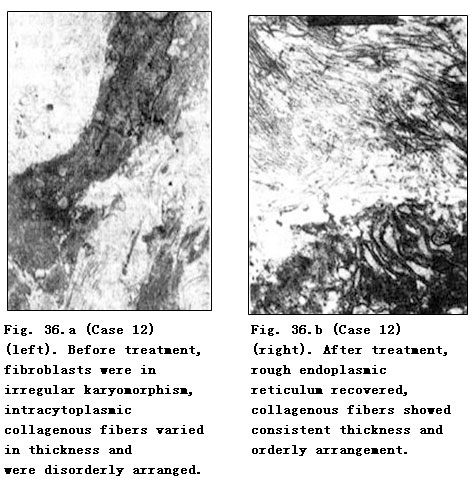
Electron Microscope: Before treatment, fibroblasts showed disrupted karyomorphism, contracted nucleoli, expanded perinuclear space and paranuclear vacuolar degeneration. A faint staining area was observed in the paranuclear margin of mussily arranged fibrocytes. Collagenous fibers varied in thickness with breaking and dissolution. After MEBO treatment, the nucleoli and nuclei of fibroblasts recovered to normal and collagenous fibers appeared to be uniform in thickness and orderly in arrangement. Master cells were occasionally visible after treatment in a few cases. Fibrocytes recovered to normal with orderly arrangement and intracytoplasmic rough endoplasmic reticulum appeared (Table 57).
CONCLUSION
Light- and electron-microscopic observations of 12 cases of deep burns wounds with granulation tissues demonstrated the dynamic comparison of histopathological alterations before and after MEBO treatment. We noted especially the changes in fibroblasts, collagenous fibers and mast cells. No uniform histological changes were observed such as are reported in the scientific literature where burns wounds were treated with conventional surgical therapy resulting in hypertrophic scarring. In our study, short-term macroscopic observation revealed that healed burns wounds formed no scars which were elevated from skin surface. This suggests that MEBO offers excellent prognosis for the treatment of deep second-degree and superficial third-degree burns wounds without scarring.
DISCUSSION
Many factors are involved in the wound healing process from trauma in general and burns wounds in particular. Among these factors, the importance of those inherent to the cell itself has been especially recognized lately by scholars [3-6]. However, when conducting research to explore the mechanism of wound healing free of hypertrophic scarring, one should attend to histopathology, in other words, try to understand the alterations of collagenous fibers, fibroblasts and mast cells [7].
In 1973 and 1974, Linares used light and electron microscopes for observation and found that hypertrophic scarring as a result of postburn granulation tissue appeared whirlpool-like or in a nodosity arrangement. In the early stage after wound healing, there were a paucity of elastic fibers initially but eventually over years a structure of lamellar or plexiform shape could be established. Mast cells took on varied shapes: round, oval or claviform with deep granular staining. These mast cells released histamine to stimulate the synthesis of collagen and also secreted many active substances to promote scar proliferation. The greater the number of mast cells in granulation tissues, the greater the likelihood of healing with hypertrophic scarring.
In 1971, using the electron microscope, Gabbiani’s group noted the presence of fibroblast-like cells in granulation tissues which correlated to wound contraction. In 1980, Rudoph demonstrated that these cells had the same ultrastructure as fibroblasts and smooth muscle cells. They named these cells myofibroblasts, the presence of which in granulation tissues predicted the possibility of hypertrophic scar formation [7, 8].
In the present study, the authors found absence of whirlpool-like or nodosity-arranged collagenous fibers and myofibroblast after MEBO treatment. Small numbers of mast cells were observed in 2 cases which are consistent with the number expected in normal skin. Research conducted by He [7] showed the existence of many more mast cells in hypertrophic scars than that in normal skin. Therefore, the light- and transmission electron-microscopic observations as well as our pictures after wound healing revealed wounds free of hypertrophic scars after MEBO treatment. Long-term effects remain to be investigated histologically as these were short-term observations.
Acknowledgments
The authors would like to thank the Electron Microscopy Department of No. 202 PLA Hospital, Burns Department, and the Basis Research Department of the General Hospital of Benxi Steel Company for technical assistance.
REFERENCES
1. Xu RX: Medical sciences on burns, wounds and ulcers. Chin J Burns Wounds Surface Ulcers 1994; 6: 45-51.
2. Zhao JX, Yang GM, Li TY, et al: Clinical analysis of 1003 burn cases treated with moist exposed burn therapy. Chin J Burns Wounds Surface Ulcers 1992; 4: 36-40.
3. Peruccio D, et al: Altered biosynthesis of tumour necrosis factor (TNF) alpha is involved in post-burn hypertrophic scars. Burns 1994; 20: 118-121.
4. Hong ST, et al: Ultrastructure of scars resulted from burns. Metal Med 1985; 1: 5-8.
5. Wang GS, Jian WG, Xu XS, et al: The exploration of pathological changes and mechanism of experimental burned rabbits after treatment with moist exposed burn ointment. Chin J Burns Wounds Surface Ulcers 1992; 4: 7~11.
6. Xi SC: Growth regulation of fibroblast. Chin J Burns Wounds Surface Ulcers 1994; 6: 5-7.
7. He GZ: Pathological changes of hypertrophic scar tissue. Chongqing Med J 1992; 21: 118-210.
8. Stephen A: Wound contraction and fibroconstractive disorders. Arch Surg 1978; 113: 1034-1046.